

Matthew E. Prekker, M.D., M.P.H., Brian E. Driver, Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults
The DirEct versus VIdeo LaryngosCopE (DEVICE) trial is a prospective, multicentre, non-blinded, randomised trial being conducted in 7 EDs and 10 ICUs in the USA
Critically ill adults undergoing tracheal intubation randomly assigned to the video-laryngoscope group or the direct-laryngoscope group
The primary outcome was successful intubation on the first attempt.
The secondary outcome was the occurrence of severe complications during intubation: severe hypoxemia, severe hypotension, new or increased vasopressor use, cardiac arrest, or death.
The trial was stopped for efficacy at the time of the single preplanned interim analysis.

Conclusions: Among critically ill adults undergoing tracheal intubation in an emergency department or ICU, the use of a videolaryngoscope resulted in a higher incidence of successful intubation on the first attempt than the use of a direct laryngoscope.
Comment: This a long journey hopefully coming to an end. From 2022 we have clear evidences on the superiority of Video versus Direct laryngoscopy Hansel J, Rogers AM, Lewis SR, Cook TM, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst Rev. 2022 Apr 4;4(4):CD011136. doi: 10.1002/14651858.CD011136.pub3. PMID: 35373840; PMCID: PMC8978307.. Main airway management societies (Difficult Airway Society; Society for Airway Management; European Airway Management Society; All India Difficult Airway Society; Canadian Airway Focus Group; Safe Airway Society; and International Airway Management Society) recently updated their statements on preventing the accidental oesophageal intubation in that sense. Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies. The DEVICE trial is another brick in the wall of consciousness about superiority of VL vs DL despite some findings are not replicable ( ex. DL FPS 70,8%) in systems where airway management and expertise in DL is a longstanding tradition. But as said we didn’t need this trial to arrive at the conclusion of the journey.
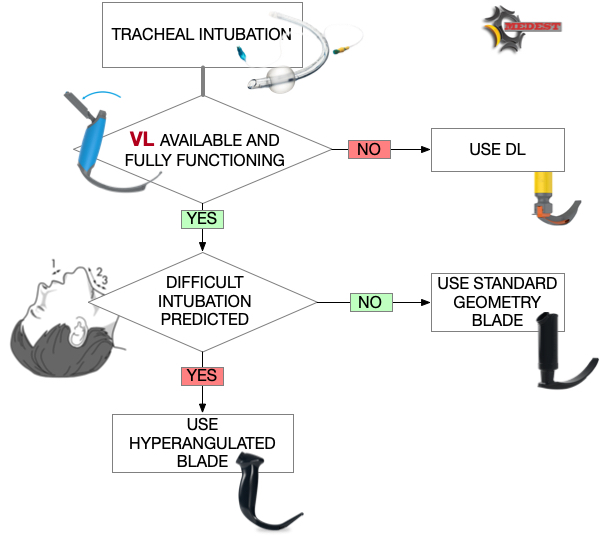
Use the videolaryngoscope (VL) as first choice in emergent tracheal intubation to improve first passage success and prevent accidental oesophageal intubation.
Use direct laryngoscope (DL) just as rescue device in case of technical failure of the videolrayngoscope
All medical systems involved in airway management need to be aware of this. A videolaryngoscope is no longer an option but a standard equipment. The best choice is to have both, standard and hyperangulated geometry blades, in adult and paediatric sizes.
The first approach with a standard geometry blade permits to shift from VL to DL without changing device. The hyparangulated blade can be useful in selected cases even as first option..
We also consequently need to shift paradigm from classical way of teaching airway management, to a VL first approach as default method and simulating any tech failure during the practical training forcing the trainee to use the DL as rescue plan.
To let me know what is your opinion fill the survey at the link below:
Also read:














Defibrillation Strategies: Why AHA’s position on VC and DSED is Controversial
1 FebNew 2025 Guidelines on Cardiopulmonary Resuscitation stated that alternative strategy for defibrillation of persistent VF/pVT are not yet ready for prime line based on the actual available evidences.
Previously ILCOR stated about the same topic: We suggest that a double sequential defibrillation strategy (weak recommendation, low certainty of evidence) or a vector change defibrillation strategy (weak recommendation, very low certainty of evidence) may be considered for adults with cardiac arrest who remain in ventricular fibrillation or pulseless ventricular tachycardia after 3 or more consecutive shocks.
So AHA degraded the ILCOR “may be considered to a “non useful” despite the same level of grade and evidences. Let’s see why and why THIS IS WRONG
AHA: It found significant improvement in survival at hospital discharge with VC and DSED compared to standard defibrillation by intention-to-treat, but notably not when trial findings were analyzed by the treatment strategy patients actually received
In summary, AHA highlighted one point for not suggesting VC or DSED over standard defibrillation. The reason is that the DOSE VF trial did not show any statistically relevant advantage in “per protocol analysis”!
I’m not a methodologist but I think that any of them can suffer of an heart attack hearing this statement! Intention to treat analysis is the core of randomization!
To summarize this concept here is a head to head compare between Intention to treat analysis VS per protocol analysis
In randomized control trials, analyzing patients “per protocol” removes the advantages of randomization. This choice degrades the study results to an observational level. So AHA statement is incorrect and the trial results are highly relevant
AHA: Furthermore, in a secondary exploratory analysis a significant survival benefit from DSD was only observed in the 17% of study patients in whom VF was incessant, and not in the vast majority (83%) of patients in whom VF recurred after a successful shock.
You can find the cited secondary analysis here: The impact of alternate defibrillation strategies on shock-refractory and recurrent ventricular fibrillation: A secondary analysis of the DOSE VF cluster randomized controlled trial. And the following are the results:
Shock-Refractory VF (n. 60)
Shock-Recurrent VF (n. 285)
In both cases, recurrent or persistent, even if not always statistically significant, DSD and VC performed much better than standard defibrillation WITH RESULTS ABSOLUTELY CLINICALLY RELEVANT ON ALL MAJOR OUTCOMES
AHA: The interval between each sequential “double” shock required for successfully terminating VF has also been shown experimentally (animal studies 10-100 Mses) and demonstrated in DOSE-VF itself (mean interval 650 Mses. ) to require a level of precision (separated by milliseconds) unlikely to be consistently achievable by manual activation of two defibrillators.
Th is totally wrong. The small ( 10- 100 Mses) cited from the guidelines refers to experimental animal study . DOSE-VF trial demonstrates statistically significant superiority to standard defibrillation. This superiority is observed with intervals >500 Msec that is absolutely replicable in clinical practice. The investigators also demonstrated the increase of advantages for shorter intervals. But, this increase is not seen at 10 Mses, which is only referred to in animal studies.
In case of VF/pVT. First approach:
If recurrent or refractory VF/pVT
Share this:
Tags: ACLS, ACR, arresto cardiaco, dual sequential defibrillition, emergency medicine, emergenza sanitaria territoriale, Guidelines, litterature review, medicina d'urgenza, medicina d'urgenza preospedaliera, refractory ventricular fibrillation, vector change defibrillation