New 2025 Guidelines on Cardiopulmonary Resuscitation stated that alternative strategy for defibrillation of persistent VF/pVT are not yet ready for prime line based on the actual available evidences.
Previously ILCOR stated about the same topic: We suggest that a double sequential defibrillation strategy (weak recommendation, low certainty of evidence) or a vector change defibrillation strategy (weak recommendation, very low certainty of evidence) may be considered for adults with cardiac arrest who remain in ventricular fibrillation or pulseless ventricular tachycardia after 3 or more consecutive shocks.
So AHA degraded the ILCOR “may be considered to a“non useful” despite the same level of grade and evidences. Let’s see why and why THIS IS WRONG
AHA:It found significant improvement in survival at hospital discharge with VC and DSED compared to standard defibrillation by intention-to-treat, but notably not when trial findings were analyzed by the treatment strategy patients actually received
In summary, AHA highlighted one point for not suggesting VC or DSED over standard defibrillation. The reason is that the DOSE VF trial did not show any statistically relevant advantage in “per protocol analysis”!
I’m not a methodologist but I think that any of them can suffer of an heart attack hearing this statement! Intention to treat analysis is the core of randomization!
To summarize this concept here is a head to head compare between Intention to treat analysis VS per protocol analysis
Approach
Statistically Strong?
Less Bias?
More Power?
Intention-to-treat
✅ Yes (most robust)
✅ Low bias
❌ Less power
Treatment / Per-protocol
❌ No (can be biased)
❌ Higher bias
✅ More power
In randomized control trials, analyzing patients “per protocol” removes the advantages of randomization. This choice degrades the study results to an observational level. So AHA statement is incorrect and the trial results are highly relevant
AHA: Furthermore, in a secondary exploratory analysis a significant survival benefit from DSD was only observed in the 17% of study patients in whom VF was incessant, and not in the vast majority (83%) of patients in whom VF recurred after a successful shock.
In both cases, recurrent or persistent, even if not always statistically significant, DSD and VC performed much better than standard defibrillation WITH RESULTS ABSOLUTELY CLINICALLY RELEVANT ON ALL MAJOR OUTCOMES
AHA: The interval between each sequential “double” shock required for successfully terminating VF has also been shown experimentally (animal studies 10-100 Mses) and demonstrated in DOSE-VF itself (mean interval 650 Mses. ) to require a level of precision (separated by milliseconds) unlikely to be consistently achievable by manual activation of two defibrillators.
Th is totally wrong. The small ( 10- 100 Mses) cited from the guidelines refers to experimental animal study . DOSE-VF trial demonstrates statistically significant superiority to standard defibrillation. This superiority is observed with intervals >500 Msec that is absolutely replicable in clinical practice. The investigators also demonstrated the increase of advantages for shorter intervals. But, this increase is not seen at 10 Mses, which is only referred to in animal studies.
DSED and VC are superior to standard defibrillation on every clinical relevant clinical outcome
DSED and VC uphold clinical advantages on both persistent and recurrent VF/pVT
When you chose DSED the interval between the 2 shocks is easily reproducible in clinical practice
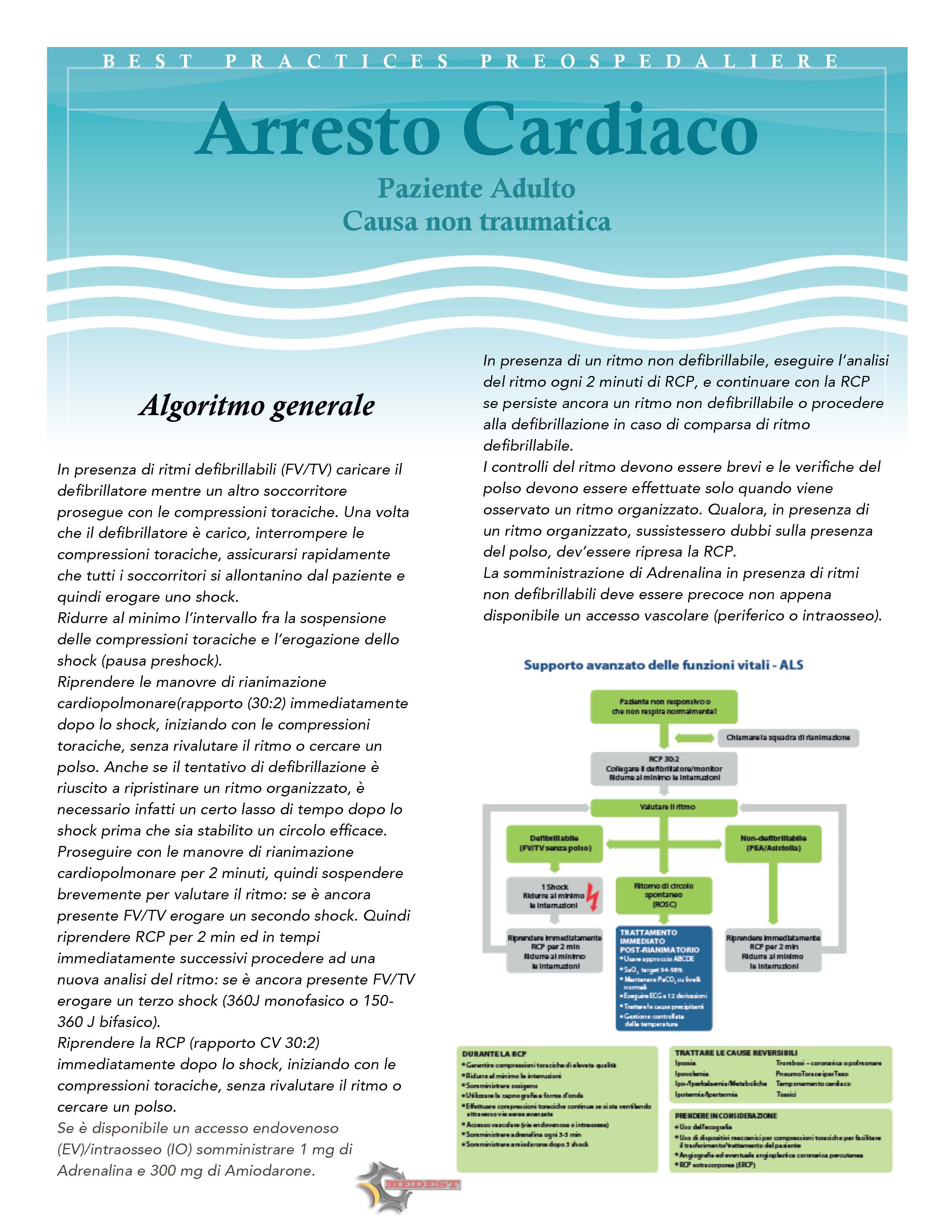
Tra tutte le “Best Practices”, quella che rappresenta più di tutte un cambio radicale di mentalità nell’approccio clinico e terapeutico, è la gestione dell’arresto cardiaco da causa traumatica. Vi prego quindi di leggere attentamente le raccomandzioni raccolte nel documento sottostante e di non esitare a esprimere le vostre riflessioni nei commenti.
ACLS Guidelines are misleading about diagnosis and treatment of pulseless electric activity (PEA) This takes to conceptual and clinical errors when treating patients in cardiac arrest. Let’s see why and if there is a better way to follow when dealing with this kind of patients. First part is about diagnosis and diagnostic tools.
Live your comment below and see you soon for Part 2. The treatment options.
Is IV tPA safe and effective for acute ischemic stroke patients if given within 3 hours of symptom onset?
Is IV tPA safe and effective for acute ischemic stroke patients treated between 3 to 4.5 hours after symptom onset?
Download and read the full policy to discover the recommendations made and based on the strength of the available data.
DISCLOSURE: MEDEST strongly encourage AWARNESS reading the propoused articles.
Abstracts are often misleading and articles potentially biased. Even this selection is not immune from potential bias (just human factors not commercial interests).
So download the full text and read it carefully to have a clear and complete opinion of the related topics.
In this episode we’ll explore the best articles of 2014 about:
Trauma
Before approaching specific arguments about trauma here are some fundamental articles to read about new emerging concepts in trauma care. Those are the clinical and physiological bases to understand what is happening in the actual trauma management scene.
After years of dogmatic approach to strict spine immobilization for all trauma patients regardless any other factor, is now pretty clear that not all the trauma patients benefits from this all or nothing way of thinking. MEDEST already faced the argument in previous posts (The Death of the Cervical Collar?) as also did some prehospital consensus guidelines (Faculty of Pre-Hospital Care Consensus Statements).
In 2014 many articles treated this topic in a critical and modern way of re-thinking spinal immobilization, in particular the widespread use of cervical collar. The lessons we learned is that:
Widespread use of cervical collar in neck trauma has to be carefully evaluated (and even avoided) due to the low incidence of unstable spinal lesions.
Routine use of cervical collar is of unclear benefit and supported by weak evidences. A new selective approach has to be implemented based on prehospital clearance protocols.
DISCLOSURE: MEDEST strongly encourage AWARNESS reading the propoused articles.
Abstracts are often misleading and articles potentially biased. Even this selection is not immune from potential bias (just human factors not commercial interests).
So download the full text and read it carefully to have a clear and complete opinion of the related topics.
The second episode of this focus reviews will deeply assess a topic that is very “hot” for every emergency professional.
Before reading this episode give a look at the first of the series about the best of 2014 literature on Cardiac Arrest
And now enjoy the very best of 2014 articles on:
Airway Management
Not all is CRASH! Especially when it comes to airway management. RSI is the gold standard when we talk about intubating a spontaneously breathin patient but DSI is becoming a classic. And is recommended by Scott Weingart and Seth Trueger, not properly two “new kids on the block”….
Caution! You are about to perform an invasive maneuver on a previously spontaneously breathing patient. So remember to carefully avoid desaturation and hyper-inflation!
This disclaimer should be written on the handle of every laryngoscope to remember two of the most frequent fault to avoid when managing the airways.
Always rewarded as a nightmare for the emergency professional, surgical airway is most of the time a real no through road for the patient. So here is a complete guide on how to approach in the best way such a difficult skill.
Does the aggressive management of the airways gets benefits on critically ill patients or a more conservative approach gives best results on clinical outcomes? Facts (few) and doubts (many) in this year literature.
DISCLOSURE: MEDEST strongly encourage AWARNESS reading the propoused articles.
Abstracts are often misleading and articles potentially biased. Even this selection is not immune from potential bias (just human factors not commercial interests).
So download the full text and read it carefully to have a clear and complete opinion of the related topics.
این سایت را به آن دکتوران و محصلین طب که شب و روز برای رفاه نوع انسان فداکاری می کنند ، جوانی و لذایذ زندگی را بدون چشمداشت به امتیاز و نفرین و آفرین قربان خدمت به بشر می کنند و بار سنگین خدمت و اصلاح را بدوش می کشند ، اهداء می کنم This site is dedicated to all Doctors and students that aver the great responsibility of People’s well-being upon their shoulders and carry on their onerous task with utmost dedication and Devotionاولین سایت و ژورنال انتــرنتی علـــمی ،تخـصصی ، پــژوهشــی و آمــوزشــی طبـــی در افغــانســـتان
Learning everything I can from everywhere I can. This is my little blog to keep track of new things medical, paramedical and pre-hospital from a student's perspective.











Defibrillation Strategies: Why AHA’s position on VC and DSED is Controversial
1 FebNew 2025 Guidelines on Cardiopulmonary Resuscitation stated that alternative strategy for defibrillation of persistent VF/pVT are not yet ready for prime line based on the actual available evidences.
Previously ILCOR stated about the same topic: We suggest that a double sequential defibrillation strategy (weak recommendation, low certainty of evidence) or a vector change defibrillation strategy (weak recommendation, very low certainty of evidence) may be considered for adults with cardiac arrest who remain in ventricular fibrillation or pulseless ventricular tachycardia after 3 or more consecutive shocks.
So AHA degraded the ILCOR “may be considered to a “non useful” despite the same level of grade and evidences. Let’s see why and why THIS IS WRONG
AHA: It found significant improvement in survival at hospital discharge with VC and DSED compared to standard defibrillation by intention-to-treat, but notably not when trial findings were analyzed by the treatment strategy patients actually received
In summary, AHA highlighted one point for not suggesting VC or DSED over standard defibrillation. The reason is that the DOSE VF trial did not show any statistically relevant advantage in “per protocol analysis”!
I’m not a methodologist but I think that any of them can suffer of an heart attack hearing this statement! Intention to treat analysis is the core of randomization!
To summarize this concept here is a head to head compare between Intention to treat analysis VS per protocol analysis
In randomized control trials, analyzing patients “per protocol” removes the advantages of randomization. This choice degrades the study results to an observational level. So AHA statement is incorrect and the trial results are highly relevant
AHA: Furthermore, in a secondary exploratory analysis a significant survival benefit from DSD was only observed in the 17% of study patients in whom VF was incessant, and not in the vast majority (83%) of patients in whom VF recurred after a successful shock.
You can find the cited secondary analysis here: The impact of alternate defibrillation strategies on shock-refractory and recurrent ventricular fibrillation: A secondary analysis of the DOSE VF cluster randomized controlled trial. And the following are the results:
Shock-Refractory VF (n. 60)
Shock-Recurrent VF (n. 285)
In both cases, recurrent or persistent, even if not always statistically significant, DSD and VC performed much better than standard defibrillation WITH RESULTS ABSOLUTELY CLINICALLY RELEVANT ON ALL MAJOR OUTCOMES
AHA: The interval between each sequential “double” shock required for successfully terminating VF has also been shown experimentally (animal studies 10-100 Mses) and demonstrated in DOSE-VF itself (mean interval 650 Mses. ) to require a level of precision (separated by milliseconds) unlikely to be consistently achievable by manual activation of two defibrillators.
Th is totally wrong. The small ( 10- 100 Mses) cited from the guidelines refers to experimental animal study . DOSE-VF trial demonstrates statistically significant superiority to standard defibrillation. This superiority is observed with intervals >500 Msec that is absolutely replicable in clinical practice. The investigators also demonstrated the increase of advantages for shorter intervals. But, this increase is not seen at 10 Mses, which is only referred to in animal studies.
In case of VF/pVT. First approach:
If recurrent or refractory VF/pVT
Share this:
Tags: ACLS, ACR, arresto cardiaco, dual sequential defibrillition, emergency medicine, emergenza sanitaria territoriale, Guidelines, litterature review, medicina d'urgenza, medicina d'urgenza preospedaliera, refractory ventricular fibrillation, vector change defibrillation