This talk was recorded live at Arezzo Cadaver Lab on June 5 2017.

In Emergency Medicine “Simplicity” is synonymous of efficiency, efficacy and reproducibility.
More the time frame is stressful more we need procedures that are efficient, efficacious and standardised, in one word SIMPLE.
Critcothyrodotomy and chest drain are procedures usually performed in high stressing scenarios and more simply they are more chance of success they have.
I don’t like complicate kits. They need training of course but even a calm and protected environment, and the middle of a street or a busy ER room aren’t nothing like that.
I don’t like blindly performed procedures but prefer trusting my own senses and sensibility when performing high invasive procedures that, mostly of the times, are a lifesaving last chance.
So this is the best way I know to perform a surgical access to the airway and to drain a highly unstable tense pneumo: using simple instruments, always present in every emergency pack, and trusting my own tactile sensitivity.

In those following videos you can see live records of the procedures. They were captured during a recent cadaver lab where I had the honour to join Jim DuCanto, Yen Chow, Carmine Della Vella and Fabrizio Tarchi in teaching airway management and clinical emergency procedures.
Hope you enjoy.
![]()

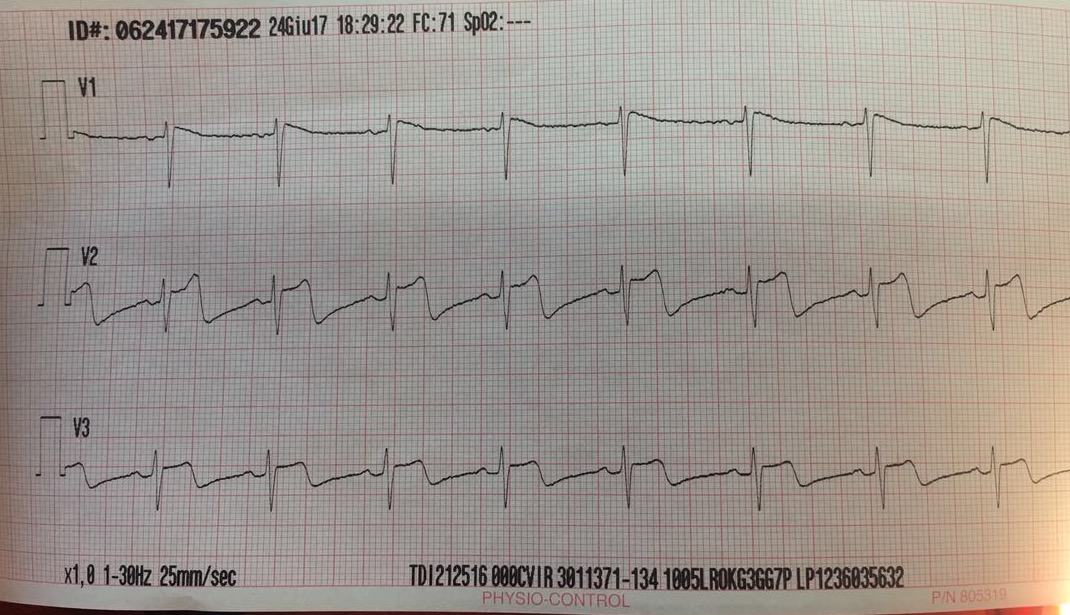
73 yrs old male found unconscious by his wife. CPR started by a neighbour with pre arrival CPR instructions provided by dispatcher. We found him in asystolic cardiac arrest. Established mechanical chest compressions (MCC), ventilated through an 8.0 ET tube, placed an intraosseus access, 10 min of ALS and 2 mg of epinephrine later, on the monitor appears an organised rhythm at 40 bpm (narrow junctional shape), NO CENTRAL PULSE. After 2 min (CPR still going) same rhythm stil NO CENTRAL PULSE but this time, during the MCC pause, a subcostal view of the heart was obtained (sorry for the quality of the images but were recorded during the code and I’m not an expert but just an ultrasound user)
As you can see the heart is moving and the right ventricle is almost the double of the left one. Due also to the clinical history of a recent surgical knee replacement the most probable origine of the cardiac arrest is PE. We decided to continue chest compressions, but to stop epinephrine at 1 mg dose, starting push doses of 0,1 mg till the return of a central pulse. After 5 min a strong carotid pulse appeared and this is the ultrasound view of the heart at that moment
The patient arrived to the hospital sedated and paralysed in assisted pressure control ventilation. You can see on the monitor the rest of vital signs.
No follow up yet.
You can read more about PEA and Pseudo-PEA on MEDEST
Forget ACLS guidelines if you are dealing with Pulseless Electric Activity. Part 1.
Forget ALS Guidelines when dealing with PEA. Part 2.
![]()


References


![]()

Kane MT. The assessment of professional competence. Eval Health Prof 1992;15:163-82.
If someone asks why a medical professional deserve to work in a public emergency medical system, despite a degree (as many others in different fields), experience (subjective) and a fist of courses (mostly individually chosen and not institutionally validated) there is nothing objective that demonstrates that this professional was, and still is, eligible for this kind of job in terms of competence.
Certification of clinical quality is something missed in action in the jungle of Health Systems in general and in Emergency Medical Services in particular.
We have generic admission criteria but no instruments to monitor on a regular basis the adequacy of clinical competence for medical professionals who work in emergency field.
We spread education, giving competences equally distributed to all medical professionals, despite any specific need.
Cultural needing are not a question of democracy.
They are specific for each person who works in a certain field and are conditioned by different personal attitudes and everyday clinical practice.
We waste time, money and human resources giving, in large part of cases, unuseful informations to the wrong persons at the wrong time of their working careers.
The fact is that we do not have a clear idea of who and which competences are needed to be a good medical emergency professional.
None stated which skills and which clinical practices, in quality and quantity, are needed to achieve a minimum level of competence.
![]()
The paradox of the demonstration of the effectiveness of the parachute with randomized controlled trials, in accordance with the method EBM (The Parachute trial), provocatively poses a fundamental question:
A 2006 article published in the BMJ Controversy Parachute approach to evidence based medicine brilliantly responded to this question.
It contains some examples of very common diseases in developing countries (HIV, dehydration in children, postpartum hemorrhage) whose remedies, implemented previously than results of relative trials where available, have saved thousands of lives.
The authors conclude that:
1. Randomised controlled trials are usually required before new interventions are implemented
2. If other evidence of effectiveness is good, and potential benefits large, the resultant delays may be unethical
3. Examples from poor countries show the price of delaying interventions
The triad of decision-making at the base of the construction of Evidenced Based Medicine provides an integrated approach between explicit data (scientific evidence derived from trials of good quality) and tacit data(clinical expertise and the patient’s needs).

The clinical decision is derived from the combination of these three factors:
• Scientific evidence
• Clinical Experience
• Needs of the patient
But when defining the level of quality of evidence those derived from clinical practice and experience are relegated to the base (lower level) of the pyramid whose apex (higher degree) are the evidence derived from studies on large patient populations.

Randomisation and de-personalization of scientific research, while eliminates everything that is “non-evident” in medical research, and is well suited to a concept of public health, on the other hand maintains an unbridgeable gap with daily clinical practice that is focused on the care of the individuals.
But in practice what we can do:
We can and we must go beyond the exclusive use of EBM in medical research and clinical practice.
The adoption of an integrated approach between the explicit scientific evidence derived from clinical trials (EBM) and a “patient- centered approach” derived from the clinical experience, should be a stimulus and an intent to the future development of our approach to the critically ill patient.
It must always be clear in the mind of the emergency medicine professionals which treatment is scientifically more correct for a given disease, but he must contextualise, and implement it for the particular patient who is dealing with at that time
![]()


Scarica la traduzione in italiano del post.
Le tue opinioni sono il nostro valore aggiunto!
Supporting ALL Ohio EM Residencies in the #FOAMed World
Let's try to make it simple
a blog for thinking docs: blending good evidence, physiology, common sense, and applying it at the bedside!
More definitive diagnosis, better patient care
Reviewing Critical Care, Journals and FOAMed
Prehospital critical care for out-of-hospital cardiac arrest
Education and entertainment for the ultrasound enthusiast
A UK PREHOSPITAL PODCAST
Emergency medicine - When minutes matter...
Sharing the Science and Art of Paediatric Anaesthesia
"Live as if you will die tomorrow; Learn as if you will live forever"
Navigating resuscitation
A Hive Mind for Prehospital and Retrieval Med
Thoughts and opinions on airways and resuscitation science
A Free Open Access Medical Education Emergency Medicine Core Content Mash Up
Rural Generalist Doctors Education
Emergency Medicine #FOAMed
این سایت را به آن دکتوران و محصلین طب که شب و روز برای رفاه نوع انسان فداکاری می کنند ، جوانی و لذایذ زندگی را بدون چشمداشت به امتیاز و نفرین و آفرین قربان خدمت به بشر می کنند و بار سنگین خدمت و اصلاح را بدوش می کشند ، اهداء می کنم This site is dedicated to all Doctors and students that aver the great responsibility of People’s well-being upon their shoulders and carry on their onerous task with utmost dedication and Devotionاولین سایت و ژورنال انتــرنتی علـــمی ،تخـصصی ، پــژوهشــی و آمــوزشــی طبـــی در افغــانســـتان
PHARM, #FOAMed
Free Open Access Medical Education
Learning everything I can from everywhere I can. This is my little blog to keep track of new things medical, paramedical and pre-hospital from a student's perspective.
In memory of Dr John Hinds
All you want to know about prehospital emergency medicine
Check out our updated blog posts at https://www.italycustomized.it/blog
The FOAM Search Engine
where everything is up for debate . . .
Pediatric Emergency Medicine Education
Free Open Access Medical Education for Paramedics
useful resources for rural clinicians
Unofficial site for prehospital care providers of the Auckland HEMS service
L'ECOGRAFIA: ENTROPIA DELL'IMMAGINE
Prehospital Emergency Medicine
Your Boot Camp Guide to Emergency Medicine
WE HAVE MOVED - VISIT WWW.KIDOCS.ORG FOR NEW CONTENT
Prehospital Emergency Medicine
Academic Medicine Pearls in Emergency Medicine from THE Ohio State University Residency Program
Prehospital Emergency Medicine
Prehospital Emergency Medicine
The Pre-Hospital & Retrieval Medicine Team of NSW Ambulance

Chest compression point. Are we compressing in the right place? Probably NOT!
8 DecThe objective of chest compressions in CPR is to compress the heart and in particular the Left Ventricle (LV) to generate a stroke volume (SV) trough the Left Ventricular Outflow Tract (LVOT) to perfuse the heart the brain and the rest of the organs.
Performing CPR we blindly compress the center of the chest on the sternum approximately at the level of intermammillar line (as recommended by the 2015 CPR Guidelines) but we risk to apply the Area of Maximum Compression (AMC) not only on the LV but also on the Aortic Valve (AV) and the Ascending Aorta (AA) closing them and generating less (or none) LV stroke volume but just an ineffective retrograde flow.
Image Attribution: Nestaas et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:54. Radiological assessment of chest compression point and achievable compression depth in cardiac patients.
Depending on how much the AMC is positioned on the left ventricle or on the aortic part of the heart chest compressions are respectively more or less efficacious to perfuse the brain the heart and the organs.
This is not just theory but was demonstrated in animal and human studies (See References links at the bottom).
In particular Sung Oh Hwang and coll. in the article “Compression of the Left Ventricular Outflow Tract During Cardiopulmonary Resuscitation” observe that”the magnitude of compression of the left ventricle is more significant when a maximal compression occurs at the LVOT than when a maximal compression occurs at the ascending aorta during external chest compression“. They also determined “that external chest compression at the hand position currently recommended by the AHA guidelines compresses the LVOT or the ascending aorta.” and conclude that “(….) the compression location currently recommended by the AHA guidelines may not be effective in generating forward blood flow during CPR.”(….) it is possible that compressing the caudal part of the sternum will improve the quality of CPR and reduce rescuer fatigue.“
The investigators stated also that the Optimal Compression Point (OCP) cannot be definitively addressed because it depends on many variables and varies from patient to patient depending “on the configuration of the heart in the thorax.”
All those findings were assessed using Trans Esophageal Echocardiography (TEE) inserted during CPR in real cases scenarios to visualise the heart to measure the LV stroke volume in order to find the best OCP.
TEE in fact is a good method to study proposition but in a short future will be a good clinical instrument to individually and visually assess the OCP, to deliver biphasic shock and to pace the heart. It is of rapid insertion in the intubated patients, is remotely and in real time monitorizza from team leader doesn’t implicate chest compressions interruption and is safe.
In another study based on a real case series “Clinical pilot study of different hand positions during manual chest compressions monitored with capnography” published in 2013, Eric Qvigstad and coll. found “that the chest compression point generating the highest EtCO2 value was evenly distributed between the patients, indicate that there is no common optimal chest com-pression point within the area tested.”
Image attribution: Qvigstad E, et al. Clinical pilot study of different hand positions during manual chest compressions monitored with capnography. Resuscitation (2013), http://dx.doi.org/10.1016/j.resuscitation.2013.03.010
They individually chosen the best hand position during chest compressions on the basis of EtCO2 values.
So which are the clinical implications for our current clinical practice?
I would like to divide the clinical take home points in two different categories:
Actual applications for clinical practice
The recommended chest compression point can be ineffective to generate enough outflow because the Area of Maximum Compression is not on the Left Ventricle but either on the Aortic Valve or the Ascending tract of the Aorta
Emergency providers can adjust the compression point based on EtCO2 values.
If, despite technically correct chest compressions, the EtCO2 remains below 10, try to adjust the compression point.
In those cases, the Optimal Compression Point is usually positioned caudally to the recommended one on the lower third of the sternum
Future development for clinical practice
TEE is a clinical useful instrument to
individually and visually assess the OCP
deliver biphasic shock
pace the heart
TEE is of rapid insertion in the intubated patients, can be remotely and in real time controlled from team leader, doesn’t implicate chest compressions interruption and is safe.
To lear more…..
Link to reference folder
Share this:
Tags: beyondguidelines, cardiac arrest, emergency medicine, emergency ultrasound, Out of Hospital Cardiac Arrest, point of care ultrasound