Quick tutorial video on simple clinical questions in prehospital emergency medicine
![]()
Quick tutorial video on simple clinical questions in prehospital emergency medicine
![]()
A debate is ongoing among #FOAMED social media about increasing first passage rate in tracheal intubation and some difficulties when using VL.
At the beginning of my experience with VL I experienced some difficulties, but with a radical change in technical approach I reached a good security on first pass success.
Here are my consideration and I hope will be useful for anyone is starting using VL
There are some fundamental differences in VL technique respect to DL, that makes the DL more easy and intuitive to pass the tube trough the cords.
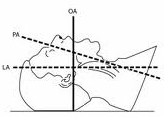
The 3 axys theory for airway management
“Sniffing position” align the pharyngeal axis with the laryngeal one

Sniffing position
Perfoming Direct Laryngoscopy with the laryngoscope we align the mouth axis to have a direct view of the cords.

DL VIEW
This view coincide with the route for passing the tube, making this step intuitive and easy.
When using a Video Laryngoscope we take our eyes right in front of the larynx, having a perfect “video” view of the vocal cords, but also minimally modifying the axis of the mouth.

VL VIEW
This difference makes the act of passing the tube not so easy and not so intuitive, cause of the contrast between the perfect video laryngeal view and the not easy passage of the tube trough the cords.
In those cases the stylet, the Bougie/Froban or the external glottic maneuvers, are useful to facilitate the video-intubation.

Golf stick shape of the tube+stylet

Epiglottoscopy is the key point of my management of the airways in general and when prforming VL in particular.
Having the epiglottis in central position on the screen allow to:
If you agree, memorize my favorite view and reach for it when using a video device to mange the airways.
All comments are welcome so please let me know your thoughts.
![]()
A novel publication goes to enrich the long-living debate on direct laryngoscopy (DL) vs video laryngoscopy (VL) efficacy in emergency intubation.
The recent article, pubblished on JEMS and titled “Deploying the Video Laryngoscope into a Ground EMS System” ,compares the success rate beetwen DL vs VL in a ground EMS Service. The device used was the King Vision with channeled blade. The partecipants had a prior training on the divide, consisting in didactic orientation and practical skills on manikins.
The result of the study shown that “Within the first 100 days of the study, the video laryngoscope utilizing the channeled blade has shown to be at least as effective as DL in relation to first-attempt success” and considering that “the mean experience in our group with DL is nine years, yet the success rate remains unacceptable” “It’s time to consider transition from a skill that’s difficult to obtain and maintain to one that appears to have a quicker learning curve and will likely result in decreased episodes of multiple attempts at intubation and associated complications.”
So is direct laryngoscopy dead?( Or will be so in a few years)

There are some fundamental differences in VL tecnique respect the DL tecnique, that makes the DL more intuitive to pass the tube trough the cords.
We have basically 3 main axis in the airways
When we manage the airways we first put the head in “sniffing position” aligning the pharyngeal axis with the laryngeal one

Then we use the laryngoscope to align the mouth axis having so a direct view of the cords. This view coincide with the way to pass the tube, making this step intitive and easy.

When using the videolaryngoscope we take our eyes right in front of the larynx, having a perfect “video” view of the vocal cords, but also minimally modifying the axis of the mouth.

For this reason passing the OTT is not straight forward, so we need the stylet, the Bougie/Froban or the external glottic maneuvers, to facilitate the intubation.

This difference in tecnique makes the VL not so intuitive due to the contrast between the perfect laryngeal view and the not intuitive passage of the tube trough the cords.
In fact the available evidences almost accordingly demonstrate an equivalent success first pass rate beetwen traditional laryngoscope an video but a prolonged intubation time in VL groups.
As the previously cited article demonstrate the learning curve for VL is short and easy to perform, and this make this tecnique surely suitable for emergency intubation.
But for emergency professionals well trained and familiar with DL I think this has to be the first choice approach when managing an emergent airway.
Emergency field is not the place to make trianing or experience with novel devices or drugs.
The still not widely availability of video-laryngoscope makes this device a perfect alternative in all the casess when is not possible to obtain a good laryngela view with DL, but still not the gold standard tecnique.
In the future the increasingly diffusion of videoleryngoscopes (due mostly to more affordable prices), will chenge the airway management scenario. Novel emergency medicine operators will grown up parallel experience wid DL and VL so the latter will be more suitable as first choice device.
Wich way you prefer to go home?
The quickest and the shorter one for sure!
Do you use the GPS to go home?
Agree, me neither!
And when you use it?

Right! When you are lost!
So that’s why Direct Laryngoscope il still my Plan A
My straight way home!

![]()
A novel publication goes to enrich the long-living debate on direct laryngoscopy (DL) vs video laryngoscopy (VL) efficacy in emergency intubation.
The recent article pubblished on JEMS “Deploying the Video Laryngoscope into a Ground EMS System” compare the success rate beetwen DL vs VL in a ground EMS Service. The device used was the King Vision with channeled blade. The partecipants had a quik training consisting in didactic orientation and practical skills on manikins.
The result of the study shown that “Within the first 100 days of the study, the video laryngoscope utilizing the channeled blade has shown to be at least as effective as DL in relation to first-attempt success” and considering that “the mean experience in our group with DL is nine years, yet the success rate remains unacceptable” “It’s time to consider transition from a skill that’s difficult to obtain and maintain to one that appears to have a quicker learning curve and will likely result in decreased episodes of multiple attempts at intubation and associated complications.”
So is direct laryngoscopy dead?( Or will be so in a few years)
Here is what I think
There are some fundamental differences in VL tecnique respect the DL tecnique, that makes the DL more intuitive to pass the tube trough the cords.
We have basically 3 main axis in the airways
When we manage the airways we first put the head in “sniffing position” aligning the pharyngeal axis with the laryngeal one
Then we use the laryngoscope to align the mouth axis having so a direct view of the cords. This view coincide with the way to pass the tube, making this step intitive and easy.
Using the videolaryngoscope we take our eyes right in front of the larynx, having a perfect “video” view of the vocal cords, but also minimally modifying the axis of the mouth.
For this reason passing the OTT is not straight forward, so we need the stylet, the Bougie/Froban or the external glottic maneuvers, to facilitate the intubation.
This difference in tecnique makes the VL a little tricky in sense of the contrast between the perfect laryngeal view and the not intuitive passage of the tube trogh the cords.
The learning curve is
So I’ll ask you:
Wich way you prefer to go home?
The quickest and the shorter one for shure!
Do you use the GPS to go home?
Agree, me neither!
And when you use it?
Right! When you are lost!
So that’s why Direct Laryngoscope il still my Plan A
My straight way home!
Prehospital Airway Management Action Plan
Le tue opinioni sono il nostro valore aggiunto!
Supporting ALL Ohio EM Residencies in the #FOAMed World
Let's try to make it simple
a blog for thinking docs: blending good evidence, physiology, common sense, and applying it at the bedside!
More definitive diagnosis, better patient care
Reviewing Critical Care, Journals and FOAMed
Prehospital critical care for out-of-hospital cardiac arrest
Education and entertainment for the ultrasound enthusiast
A UK PREHOSPITAL PODCAST
Emergency medicine - When minutes matter...
Sharing the Science and Art of Paediatric Anaesthesia
"Live as if you will die tomorrow; Learn as if you will live forever"
Navigating resuscitation
A Hive Mind for Prehospital and Retrieval Med
Thoughts and opinions on airways and resuscitation science
A Free Open Access Medical Education Emergency Medicine Core Content Mash Up
Rural Generalist Doctors Education
Emergency Medicine #FOAMed
این سایت را به آن دکتوران و محصلین طب که شب و روز برای رفاه نوع انسان فداکاری می کنند ، جوانی و لذایذ زندگی را بدون چشمداشت به امتیاز و نفرین و آفرین قربان خدمت به بشر می کنند و بار سنگین خدمت و اصلاح را بدوش می کشند ، اهداء می کنم This site is dedicated to all Doctors and students that aver the great responsibility of People’s well-being upon their shoulders and carry on their onerous task with utmost dedication and Devotionاولین سایت و ژورنال انتــرنتی علـــمی ،تخـصصی ، پــژوهشــی و آمــوزشــی طبـــی در افغــانســـتان
PHARM, #FOAMed
Free Open Access Medical Education
Learning everything I can from everywhere I can. This is my little blog to keep track of new things medical, paramedical and pre-hospital from a student's perspective.
In memory of Dr John Hinds
All you want to know about prehospital emergency medicine
Check out our updated blog posts at https://www.italycustomized.it/blog
The FOAM Search Engine
where everything is up for debate . . .
Pediatric Emergency Medicine Education
Free Open Access Medical Education for Paramedics
useful resources for rural clinicians
Unofficial site for prehospital care providers of the Auckland HEMS service
L'ECOGRAFIA: ENTROPIA DELL'IMMAGINE
Prehospital Emergency Medicine
Your Boot Camp Guide to Emergency Medicine
WE HAVE MOVED - VISIT WWW.KIDOCS.ORG FOR NEW CONTENT
Prehospital Emergency Medicine
Academic Medicine Pearls in Emergency Medicine from THE Ohio State University Residency Program
Prehospital Emergency Medicine
Prehospital Emergency Medicine
The Pre-Hospital & Retrieval Medicine Team of NSW Ambulance

God save the King!
27 JunMatthew E. Prekker, M.D., M.P.H., Brian E. Driver, Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults
The DirEct versus VIdeo LaryngosCopE (DEVICE) trial is a prospective, multicentre, non-blinded, randomised trial being conducted in 7 EDs and 10 ICUs in the USA
Critically ill adults undergoing tracheal intubation randomly assigned to the video-laryngoscope group or the direct-laryngoscope group
The primary outcome was successful intubation on the first attempt.
The secondary outcome was the occurrence of severe complications during intubation: severe hypoxemia, severe hypotension, new or increased vasopressor use, cardiac arrest, or death.
The trial was stopped for efficacy at the time of the single preplanned interim analysis.
Conclusions: Among critically ill adults undergoing tracheal intubation in an emergency department or ICU, the use of a videolaryngoscope resulted in a higher incidence of successful intubation on the first attempt than the use of a direct laryngoscope.
Comment: This a long journey hopefully coming to an end. From 2022 we have clear evidences on the superiority of Video versus Direct laryngoscopy Hansel J, Rogers AM, Lewis SR, Cook TM, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst Rev. 2022 Apr 4;4(4):CD011136. doi: 10.1002/14651858.CD011136.pub3. PMID: 35373840; PMCID: PMC8978307.. Main airway management societies (Difficult Airway Society; Society for Airway Management; European Airway Management Society; All India Difficult Airway Society; Canadian Airway Focus Group; Safe Airway Society; and International Airway Management Society) recently updated their statements on preventing the accidental oesophageal intubation in that sense. Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies. The DEVICE trial is another brick in the wall of consciousness about superiority of VL vs DL despite some findings are not replicable ( ex. DL FPS 70,8%) in systems where airway management and expertise in DL is a longstanding tradition. But as said we didn’t need this trial to arrive at the conclusion of the journey.
Use the videolaryngoscope (VL) as first choice in emergent tracheal intubation to improve first passage success and prevent accidental oesophageal intubation.
Use direct laryngoscope (DL) just as rescue device in case of technical failure of the videolrayngoscope
All medical systems involved in airway management need to be aware of this. A videolaryngoscope is no longer an option but a standard equipment. The best choice is to have both, standard and hyperangulated geometry blades, in adult and paediatric sizes.
The first approach with a standard geometry blade permits to shift from VL to DL without changing device. The hyparangulated blade can be useful in selected cases even as first option..
We also consequently need to shift paradigm from classical way of teaching airway management, to a VL first approach as default method and simulating any tech failure during the practical training forcing the trainee to use the DL as rescue plan.
To let me know what is your opinion fill the survey at the link below:
VL first approach
Also read:
Share this:
Tags: advanced airway management, Airway management, emergency medicine, litterature review, medicina d'urgenza, prehospital emergency medicine, videolaryngoscopy