New 2025 Guidelines on Cardiopulmonary Resuscitation stated that alternative strategy for defibrillation of persistent VF/pVT are not yet ready for prime line based on the actual available evidences.
Previously ILCOR stated about the same topic: We suggest that a double sequential defibrillation strategy (weak recommendation, low certainty of evidence) or a vector change defibrillation strategy (weak recommendation, very low certainty of evidence) may be considered for adults with cardiac arrest who remain in ventricular fibrillation or pulseless ventricular tachycardia after 3 or more consecutive shocks.
So AHA degraded the ILCOR “may be considered to a“non useful” despite the same level of grade and evidences. Let’s see why and why THIS IS WRONG
AHA:It found significant improvement in survival at hospital discharge with VC and DSED compared to standard defibrillation by intention-to-treat, but notably not when trial findings were analyzed by the treatment strategy patients actually received
In summary, AHA highlighted one point for not suggesting VC or DSED over standard defibrillation. The reason is that the DOSE VF trial did not show any statistically relevant advantage in “per protocol analysis”!
I’m not a methodologist but I think that any of them can suffer of an heart attack hearing this statement! Intention to treat analysis is the core of randomization!
To summarize this concept here is a head to head compare between Intention to treat analysis VS per protocol analysis
Approach
Statistically Strong?
Less Bias?
More Power?
Intention-to-treat
✅ Yes (most robust)
✅ Low bias
❌ Less power
Treatment / Per-protocol
❌ No (can be biased)
❌ Higher bias
✅ More power
In randomized control trials, analyzing patients “per protocol” removes the advantages of randomization. This choice degrades the study results to an observational level. So AHA statement is incorrect and the trial results are highly relevant
AHA: Furthermore, in a secondary exploratory analysis a significant survival benefit from DSD was only observed in the 17% of study patients in whom VF was incessant, and not in the vast majority (83%) of patients in whom VF recurred after a successful shock.
In both cases, recurrent or persistent, even if not always statistically significant, DSD and VC performed much better than standard defibrillation WITH RESULTS ABSOLUTELY CLINICALLY RELEVANT ON ALL MAJOR OUTCOMES
AHA: The interval between each sequential “double” shock required for successfully terminating VF has also been shown experimentally (animal studies 10-100 Mses) and demonstrated in DOSE-VF itself (mean interval 650 Mses. ) to require a level of precision (separated by milliseconds) unlikely to be consistently achievable by manual activation of two defibrillators.
Th is totally wrong. The small ( 10- 100 Mses) cited from the guidelines refers to experimental animal study . DOSE-VF trial demonstrates statistically significant superiority to standard defibrillation. This superiority is observed with intervals >500 Msec that is absolutely replicable in clinical practice. The investigators also demonstrated the increase of advantages for shorter intervals. But, this increase is not seen at 10 Mses, which is only referred to in animal studies.
DSED and VC are superior to standard defibrillation on every clinical relevant clinical outcome
DSED and VC uphold clinical advantages on both persistent and recurrent VF/pVT
When you chose DSED the interval between the 2 shocks is easily reproducible in clinical practice
Critically ill adults undergoing tracheal intubation randomly assigned to the video-laryngoscope group or the direct-laryngoscope group
The primary outcome was successful intubation on the first attempt.
The secondary outcome was the occurrence of severe complications during intubation: severe hypoxemia, severe hypotension, new or increased vasopressor use, cardiac arrest, or death.
The trial was stopped for efficacy at the time of the single preplanned interim analysis.
Conclusions: Among critically ill adults undergoing tracheal intubation in an emergency department or ICU, the use of a videolaryngoscope resulted in a higher incidence of successful intubation on the first attempt than the use of a direct laryngoscope.
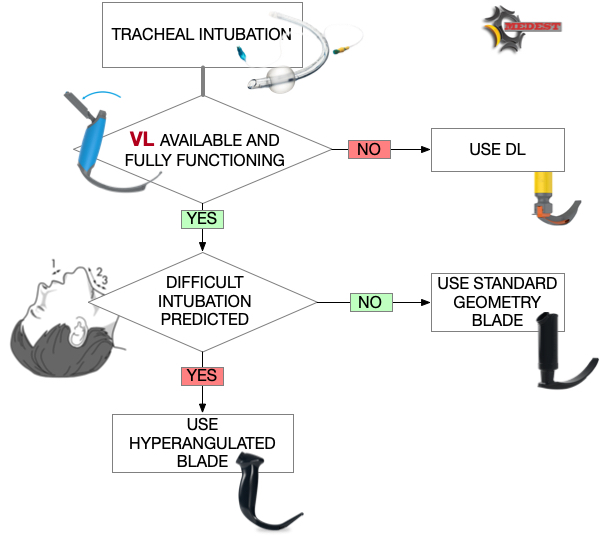
Use the videolaryngoscope (VL) as first choice in emergent tracheal intubation to improve first passage success and prevent accidental oesophageal intubation.
Use direct laryngoscope (DL) just as rescue device in case of technical failure of the videolrayngoscope
All medical systems involved in airway management need to be aware of this. A videolaryngoscope is no longer an option but a standard equipment. The best choice is to have both, standard and hyperangulated geometry blades, in adult and paediatric sizes.
The first approach with a standard geometry blade permits to shift from VL to DL without changing device. The hyparangulated blade can be useful in selected cases even as first option..
We also consequently need toshift paradigm from classical way of teaching airway management, to a VL first approach as default method and simulating any tech failure during the practical training forcing the trainee to use the DL as rescue plan.
To let me know what is your opinion fill the survey at the link below:
You arrive on the scene of a motorbike accident. The driver, a 50 years old male, at your arrival is in “Pain” state with eyes closed and you can hear just a “snoring” sound coming from his mouth. His vitals are: NIMBP 80 over 50, HR 110, A quick primary survey reveal a low level of consciousness (eyes closed no finalised arms movement) with restored airway patency that after basic airway manoeuvres and O2 therapy (SaO2 goes to 95%) no signs of tension pneumo. A quick look to the pelvis and legs reveal a suspected “open book” lesion and a bilateral femoral fracture. No PMH is available at the moment.
Physiological response to shock
From the primary survey and vitals you can understand the patient is compensating a state of profound (hypovolemic) shock and consequent organ low perfusion with a sympathetic activation. Endogenous adrenergic mediators are trying to restore organ perfusion by vasoconstriction and increase in cardiac output.
First do not harm
Can we kill a patient destroying the physiologic response to shock?
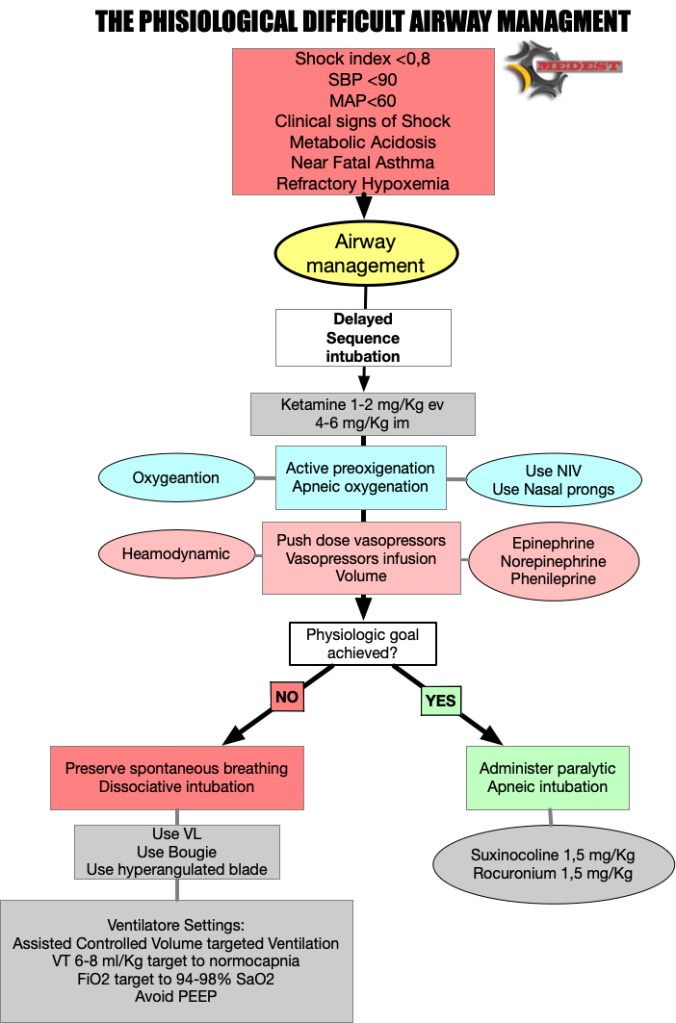
The answer is YES! The need to protect airway performing a rapid pharmacological assisted airway management (RSI), can lead to bad consequences, destroying the physiological response to a state of profound shock.
All sedative, analgesic and anaesthetic drugs in fact antagonise and depress the sympathetic adrenergic response physiologically targeted to restore perfusion to vital organs.
First do not harm and choose minimal emodynamic impact type and dose of drugs to perform sedation. As we know (till now) the better choice are Ketamine and Etomidate with no clear evidences on which one is preferable. We for sure know that Ketamine can be dangerous in cathecolamine depleted patients and that this effect is dose dependent. So consider using a lower dose to reach dissociative threshold being conscious that can lead to a non ideal intubation condition.
After a dissociative dose of Ketamine, our next clinical target is to reanimate the patient form an oxygenation and/or an organ perfusion point of view.
So we shift from a concept of Rapid Sequence Intubation to a more comprehensive plan of Delayed Sequence Airway Management. Delayed (Ketamine/Etomidate induced) to get time and reanimate, Airway Management intended as any plan (tracheal intubation, supraglottic airway) we can apply in that specific patient in the middle of the road or in other prehospital scenarios.
A properly performed pre-oxygenation with the adjunct of apneic oxygenation can restore O2 levels giving us also a good reserve for following apnea times.
Cautelative fluid administration (avoid fluids in trauma, use BLOOD) and, push dose (Epinephrine, Phenilephrine) or continuous infusion (Norepinephrine)vasopressors, can restore perfusion to abdominal and extra abdominal organs by increasing circulating volume and cardiac performance (Alfa and Beta agonist ).
Delayed paralytic administration give us the time to perform a proper reanimation reanimation and to check the effects of our interventions.
If everything goes well and the patient’s oxygenation and emodynamic state is compensated, we can administer paralytic, and go straight to perform tracheal intubation.
But if the patient remains uncompensated despite all our efforts to correct the potentially lethal cause, our last weapon can be to preserve spontaneous breathing.
Don’t live me breathless
WHY? During inspiratory phase of respiratory cycle the negative intrathoracic pressure favourites venous return and increase the telediastolic volume of the left ventricle. The augmented left ventricle end diastolic pressure (LVEDP) according to Frank-Starling law improves myocardial performance increasing stroke volume and consequently cardiac output.
The refractory shocked patient is heavily preload dependent and suppressing the inspiratory drive risk to worsen the already dramatic emodynamic state taking him on the irreversible part of the shock curve.
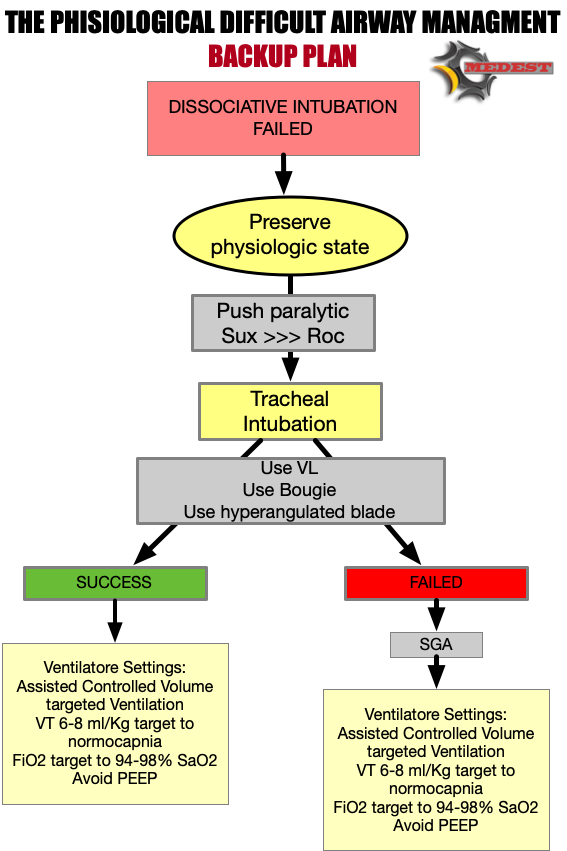
We’ve got a plan
We need to have a plan for high difficult physiological airways. This is just a small residual percentage of the airways we manage in our clinical practice, but can be dramatically catastrophic when we deal with those patients without a precise plan.
We’ve got a backup plan
But when intubation fails we need to have a backup plan!
Case conclusion
You understand the need to protect patient’s airways but also the extreme physiologic difficulty of this airway.
After administering a dissociative dose of Ketamine, due to the failure of any try to restore perfusion, you decide to perform a DISSOCIATIVE INTUBATION using a videolaryngoscope with a hyperangulated blade and a bougie, AVOIDING PARALYSIS.
Then you put the patient on ACV mechanical ventilation targeting a TV of 6 ml/kg and considering a “zero PEEP” strategy.
Special Thanks to Scott Weingart and Jim DuCanto for the kindness and fundamental mentorship on inspiring and peer reviewing the algorithm
Chest compressions alternate to abdominal compression–decompression technique
Background
The abdominal compression–decompression technique is based on an “abdominal pump” model, which induces pressure changes within the abdominal cavity and promotes the return of blood from the abdominal cavity to fill the heart and be eventually pumped to the brain. A combination of abdominal compression–decompression and chest compression was previously shown to increase the venous refilling of the heart, which could generate increased coronary perfusion pressure and increase blood flow to vital organs . With this combination method, chest release during abdominal compression leads to increased venous return to the thorax by negative intrathoracic pressure. Moreover, abdominal decompression during chest compression may lead to increased blood flow via decreased afterload. In myocardial blood flow, a better 48-h outcome was documented with the combination method compared with STD-CPR
This study was performed in China. It’s a single center, randomised, not blinded study.
The study aimed to compare the outcomes of standard cardiopulmonary resuscitation (STD- CPR) and combined chest compression and abdominal compression–decompression cardiopulmonary resuscitation (CO-CPR) following out-of-hospital cardiac arrest (OHCA).
Primary outcome ROSC. Secondary outcome hospital admission, hospital discharge and neurological outcome at hospital discharge.
Results
ROSC and survival to hospital admission: no statistical benefit
Survival at hospital discharge and neurological outcome: CO-CPR had statistical significant better outcome respect STD-CPR
Limitations
Single center, small sample size, no evaluation of possible abdominal injuries.
Bottom line
For prehospital use of combined chest compression and abdominal compression–decompression cardiopulmonary resuscitation we have first of all to account the need of an additional rescuer to perform abdominal compression-decompression. By the way the alternate chest/abdominal compression-decompression method is promising even if we need larger multicenter randomised trial for a more consistent evaluation of its efficacy.
Head and thorax elevation during cardiopulmonary resuscitation
Background
Gradual elevation of the head and thorax enhances venous return from the head and neck to the thorax and further lowers intracranial pressure. This automated controlled elevation (ACE) CPR strategy consists of: (1) manual active compression decompression (ACD)-CPR and/or suction cup-based automated (LUCAS 3) CPR; (2) an impedance threshold device (ITD); and (3) an automated controlled head and thorax patient positioning device (APPD).
Observational, prospective study. The Objectives of the study was to assess the probability of OHCA survival to hospital discharge after ACE-CPR versus C-CPR. ACE-CPR data were collected from a dedicated registry implemented by 10 EMS Agencies. Conventional (C) CPR data were collected from 3 large historical randomized controlled OHCA resuscitation trials.
NB: for ACE-CPR only 6/10 agencies data were evaluated.
The primary outcome was survival to hospital discharge. Secondary outcomes included ROSC at any time, and survival to hospital dis- charge with favorable neurological function.
Results
Cumulative results on primary and secondary outcome before taking into consideration the time from 911 call to ACE-CPR were not statistically significative differences. The statistical significance of ACE-CPR was reached only when time from 911 call to ACE-CPR initiation was considered.
Limitations
Observational study. Participating personnel form EMS agencies were highly motivated about ACE-CPR. 165 patients excluded with no clear explanation (generally didn’t meet inclusion criteria) from 4 EMS participating agencies. Statistical significance on primary and secondary outcome was reached after surrogate secondary analysis that considered time form 911 call to ACE-CPR start.
Bottom line
There are still insufficient historical data to understand the benefit of automated controlled elevation (ACE) CPR and this study doesn’t clear any doubt about it’s efficacies on clinical oriented outcomes.
Aortic occlusion during cardiac arrest. Mechanical adrenaline?
Background
Thoracic aortic occlusion during chest compressions limits the vascular bed for the generated cardiac output. This may increase the aortic pressure and subsequently the coronary perfusion pressure (CPP).
The coronary perfusion pressure (CPP), the pressure gradient between the aorta and right atrium, is a major determinant of the myocardial blood flow. Consequently, generating a high CPP by providing high-quality chest compression during CPR is one of the most critical factors for achieving ROSC in cardiac arrest patients.
It is uncontroversial to state that the desired effect of adrenaline in CPR is the potential increase in CPP. The potential detrimental effects of adrenaline, such as decreased cerebral blood flow, increased myocardial oxygen consumption or recurrent ventricular tachycardias after ROSC, is yet to be found with REBOA. However, adverse effects of REBOA are not reported in the limited human data published, nor has this been an endpoint in the studies conducted so far.
This is a pilot study. The aim of the study was to calculate the CPP before and after REBOA balloon inflation. EtCO2 and median aortic pressure before and after balloon inflating were also measured.
Results
CPP, MAP and EtCO2 significative increased after REBOA placement in Zone 1 and balloon inflation
Limitations
Single center, small numbers, need of a large number of operators to insert the REBOA and to obtain the measurements.
Bottom line
REBOA in Cardiac Arrest is potentially useful to increase CPP and less dangerous than epinephrine administration.
It’s feasibility in emergency (in-hospital and out of hospital) settings in a timely manner and with a small number of medical personnel needs to be demonstrated.
Thanks to a prestigious panel of international authors. Great job and definitely solid indication about how to prevent and recognise accidental oesophageal intubation.
Just some of the key recommendations
Exhaled carbon dioxide monitoring and pulse oximetry should be available and used for all episodes of airway management.
Routine use of a videolaryngoscope is recommended whenever feasible.
Inability to detect sustained exhaled carbon dioxide requires oesophageal intubation to be actively excluded.
Tube removal should be undertaken if any of the following are true:
Oesophageal placement cannot be excluded
Sustained exhaled carbon dioxide cannot be restored
Oxygen saturation deteriorates at any point before restoring sustained exhaled carbon dioxide
The following are personal considerations on peculiar aspects about management of accidental oesophageal intubation in prehospital environment and come from my personal clinical experience.
Beware they are just personal considerations and practical tricks and tips and are not intended to substitute the above guidelines.
They are intended to suggest an alternative mental and technical approach when dealing with oesophageal intubation on uncontrolled patients in difficult environment.
Some general considerations
Prehospital uncontrolled patients are not on empty stomach so are at high risk of regurgitation/inhalation
Even few ventilation efforts in case of oesophageal intubation pone the patient at high risk of regurgitation/inhalation
Suctioning in prehospital setting is not always ready avalliate (mind your environment) or maximally performant (mind your equipment)
First attempt in prehospital setting must be always the best one. Think before trying a second attempt in case of failure. Implement your plan or change plan.
Apply the Indication, Suitability, Feasibility approach while supporting oxygenation, ventilation and protection.
DO NOT REMOVE THE OT TUBE STRAIGHT FORWARD IN CASE OF ACCIDENTAL OESOPHAGEAL INTUBATION IN PREHOSPITAL ENVIRONMENT.
The way I like it. The way I do it.
Live the “oesophageal” OT tube in (overcuffed) and if it’s possible apply a continuous suctioning to exclude the oesophagus and protect the airways
Place a SGA to restore oxygenation and ventilation (trough BMV or NIV)
After restoring oxygenation (SaO2 >94%) and ventilation (EtCO2 40 mmHg) if suitable and feasible (see below) proceed to a second attempt of tracheal intubation (must be videolaryngoscope+bougie)
If the second attempt succeeds remove the “oesophageal” OT
If the second attempt is not suitable or feasible transport to nearest hospital (patient is well oxygenated and ventilated via SGA and protected via oesophageal exclusion) for further stabilisation (you can replace the oesophageal OT tube with a large bore oro-gastric tube or insert the orogastric tube trough the SGA dedicated channel)
If you can’t restore oxygenation and ventilation via SGA or you can’t place a SGA remove the oesophageal OT tube and try to oxygenate and ventilate (remember patient is not protected) via BVM and NC (double oxygenation)
If even BVM fails declare CICO
Suitability
Do I have a plan to implement regarding the first attempt
Can I improve my environment (Setting) moving the patient to a more comfortable place/position
Is the time to nearest hospital short/long
Feasibility
Am I in the right mental mood after 1st attempt (me) to try a better second one
Is my team ready for a second attempt (team)
Do I have the right equipment to implement my second attempt (Equipment)
این سایت را به آن دکتوران و محصلین طب که شب و روز برای رفاه نوع انسان فداکاری می کنند ، جوانی و لذایذ زندگی را بدون چشمداشت به امتیاز و نفرین و آفرین قربان خدمت به بشر می کنند و بار سنگین خدمت و اصلاح را بدوش می کشند ، اهداء می کنم This site is dedicated to all Doctors and students that aver the great responsibility of People’s well-being upon their shoulders and carry on their onerous task with utmost dedication and Devotionاولین سایت و ژورنال انتــرنتی علـــمی ،تخـصصی ، پــژوهشــی و آمــوزشــی طبـــی در افغــانســـتان
Learning everything I can from everywhere I can. This is my little blog to keep track of new things medical, paramedical and pre-hospital from a student's perspective.






















Defibrillation Strategies: Why AHA’s position on VC and DSED is Controversial
1 FebNew 2025 Guidelines on Cardiopulmonary Resuscitation stated that alternative strategy for defibrillation of persistent VF/pVT are not yet ready for prime line based on the actual available evidences.
Previously ILCOR stated about the same topic: We suggest that a double sequential defibrillation strategy (weak recommendation, low certainty of evidence) or a vector change defibrillation strategy (weak recommendation, very low certainty of evidence) may be considered for adults with cardiac arrest who remain in ventricular fibrillation or pulseless ventricular tachycardia after 3 or more consecutive shocks.
So AHA degraded the ILCOR “may be considered to a “non useful” despite the same level of grade and evidences. Let’s see why and why THIS IS WRONG
AHA: It found significant improvement in survival at hospital discharge with VC and DSED compared to standard defibrillation by intention-to-treat, but notably not when trial findings were analyzed by the treatment strategy patients actually received
In summary, AHA highlighted one point for not suggesting VC or DSED over standard defibrillation. The reason is that the DOSE VF trial did not show any statistically relevant advantage in “per protocol analysis”!
I’m not a methodologist but I think that any of them can suffer of an heart attack hearing this statement! Intention to treat analysis is the core of randomization!
To summarize this concept here is a head to head compare between Intention to treat analysis VS per protocol analysis
In randomized control trials, analyzing patients “per protocol” removes the advantages of randomization. This choice degrades the study results to an observational level. So AHA statement is incorrect and the trial results are highly relevant
AHA: Furthermore, in a secondary exploratory analysis a significant survival benefit from DSD was only observed in the 17% of study patients in whom VF was incessant, and not in the vast majority (83%) of patients in whom VF recurred after a successful shock.
You can find the cited secondary analysis here: The impact of alternate defibrillation strategies on shock-refractory and recurrent ventricular fibrillation: A secondary analysis of the DOSE VF cluster randomized controlled trial. And the following are the results:
Shock-Refractory VF (n. 60)
Shock-Recurrent VF (n. 285)
In both cases, recurrent or persistent, even if not always statistically significant, DSD and VC performed much better than standard defibrillation WITH RESULTS ABSOLUTELY CLINICALLY RELEVANT ON ALL MAJOR OUTCOMES
AHA: The interval between each sequential “double” shock required for successfully terminating VF has also been shown experimentally (animal studies 10-100 Mses) and demonstrated in DOSE-VF itself (mean interval 650 Mses. ) to require a level of precision (separated by milliseconds) unlikely to be consistently achievable by manual activation of two defibrillators.
Th is totally wrong. The small ( 10- 100 Mses) cited from the guidelines refers to experimental animal study . DOSE-VF trial demonstrates statistically significant superiority to standard defibrillation. This superiority is observed with intervals >500 Msec that is absolutely replicable in clinical practice. The investigators also demonstrated the increase of advantages for shorter intervals. But, this increase is not seen at 10 Mses, which is only referred to in animal studies.
In case of VF/pVT. First approach:
If recurrent or refractory VF/pVT
Share this:
Tags: ACLS, ACR, arresto cardiaco, dual sequential defibrillition, emergency medicine, emergenza sanitaria territoriale, Guidelines, litterature review, medicina d'urgenza, medicina d'urgenza preospedaliera, refractory ventricular fibrillation, vector change defibrillation