
Clinical Scenario
55 years old male arrested in front of the ACLS team in prehospital setting.
The call was due to hypotension and cold sweeting. The team found the patient conscious and responding to their answers. He denied chest pain or dyspnea, referring just dizziness and profound astenia.
No time to put him on monitor and BOOM! Cardiac arrest occurred. PEA. Narrow organised EKG activity, no carotid pulse no indirect signs of circulation.
Mechanical CPR and standard ACLS started. First rhythm control, probe on the chest (subxifoid view)
HEART IS MOVING! NO CAROTID PULSE YET. This is not a cardiac arrest, but it’s not ROSC either!
What’s this condition? For standard ACLS it doesn’t exists, it’s not mentioned and there are no practice guidelines to follow.
But beyond ACLS this is a well recognised situation and is called PSEUDO PEA.
Pseudo PEA
In a recent trial (Focused echocardiographic evaluation in life support and peri-resuscitation of emergency patients: a prospective trial link in the references) evaluating the use of POCUS in extreme shock and cardiac arrest in prehospital setting the investigators found that, examining with ultrasound patients in cardiac arrest, 74,5% and 35% of PEA and Asystole respectively had cardiac wall motion and a rate of survival significatively higher than “no cardiac activity patients” (55% vs 8% in PEA and 24% vs 11% in Asystole)

Image attribution How Do You FEEL About Echo in Cardiac Arrest?
Three simple steps to manage pseudo PEA
Let’s go back to the clinical case (just to mention this is not a simulated scenario, the patient was real and the team was not from another part of the planet but was my team) How you manage this patient beyond and in absence of clear guidelines?
- Looking for reversible causes
- Monitoring perfusion
- Supporting circulation
Looking for reversible causes
Searching for reversible causes of PEA is a mix between clinical history, physical exams and instrumental findings. I’m not a great fan of H’s and T’s approach.
I use ultrasound!
If you can find the cause, treat it right away, other ways go to next steps monitoring perfusion and supporting circulation.
Monitoring perfusion
Monitoring perfusion in an arrested (technically but not practically) patient on the field (where you don’t have the chance to insert an arterial line to have invasive determination of arterial blood pressure) is a matter of indirect signs and numbers.
“The digitomer” for sure is the worst way to do it. So forget the central pulse it’s subjective and not reliable, as any BLS provider knows.
EtCO2 and pletismographic waveform of capillary pulse are both crucial elements to decide when stopping (or not stopping) CPR and starting vasopressors.
We alla know almost everything about EtCO2 and its value to show perfusion, so I want just to spend some words on a less famous, and widely underestimated, method of monitoring distal perfusion: capillary pulse waveform. We all have pulse ox, few of us consider it’s waveform at all, and certainly not as indicator of perfusion. But a wide range of recent letterature indicates a good correlation between arterial pressure and capillary pressure.
Below you can see the an analysis of the arterial pressure waveform.

Image attribution University College London (UCL) https://doi.org/10.1017/CBO9781139226394.035
and this below is the waveform recorded from a human photoplethysmogram (in other words the waveform shown from any pulse ox) at the capillary level

Image attribution https://www.sciencedirect.com/science/article/pii/S0960077915001344
We don’t need much of evidences to understand how the two waveforms correlates.
So pulse ox waveform can be used as good estimation of arterial pressure and distal perfusion even if we know its often influenced by artefacts expecially in low flow conditions.
I personally consider the EKG trace also a useful tool. An organised electric activity with narrow complexes at a normal rate is more probable to give a perfusing flow than a bradicardic, wide QRS one.
But let’s go back to practical. Which one is the best method to use in prehospital? I personally use all the information, cause in a difficult setting relying on just one of them is dangerous.
So a pseudo PEA condition with narrow complexes electric activity at a rate above 60 bpm, EtCO2 around 35-40 mmHg a good shaped capillary waveform in absence of chest compressions for me is grant of perfusion.
A non organised or wide complexes low rate ekg trace, low EtCO2 and no capillary waveform is a non perfusing state.
Supporting circulation
What to do in those cases?
In the case of “non perfusing” pseudo PEA, no doubt, you need to continue chest compressions to sustain circulatory state.
In the case of “perfusing” pseudo PEA, use vasopressors.
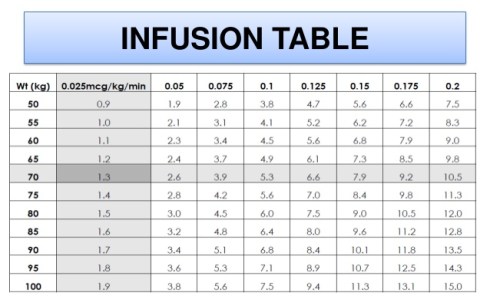
My favourite way to give them, and the more reliable in prehospital environment, is push dose.
My favorite vasopressor is Epinephrine.

Other acceptable alternative is Phenylephrine.

I don’t believe that administering vasopressors in continuous infusion on the field is a good idea. For me is dangerous and not practical. Most of the times we don’t have volumetric or infusion pump ready available so we are not sure about the exact dose administered easily loosing control of the situation.
But in case you intend to give continuous infusion vasopressors use Norepinephrine.

Conclusions
When you have a pseudo PEA patient, the crucial decision is if the present cardiac activity is perfusing (the brain and the other vital organs or not) even in absence of a palpable carotid central pulse.
To understand how is the perfusion going use EtCO2, waveform pulse oximetry and EKG.
If the signs of perfusion are not good continue with chest compressions
If you have good signs of perfusion start vasopressors to sustain circulation.
Remember: This is not an arrested patient! Needs to be in the hospital ASAP to start ECMO, PCA or other definitive care.
Take home points about pseudo PEA:
- ALWAYS use ultrasound to determine cardiac activity in cardiac arrest patients
- Don’t trust central pulse palpation
- Pseudo PEA is an ultrasound evident cardiac activity without carotid pulse
- Pseudo PEA is a big clinical reality beyond ACLS mantras
- Use ultrasound to look for reversible causes of pseudo PEA.
- Use waveform EtCO2 and waveform Pulse Oximetry to monitor perfusion
- Continue CHEST COMPRESSIONS in pseudo PEA with bad perfusion state indicators:
- Wide bradycardic electric activity
- Low EtCO2 (below 20 mmHg)
- No waveform on Pulse ox
- Use VASOPRESSORS in pseudo PEA with good perfusion state indicators:
- Narrow normofrequent electric activity
- EtCO2 above 35-40
- Good waveform on Pulse ox
References
- Breitkreutz R et al. Focused echocardiographic evaluation in life support and peri-resuscitation of emergency patients: a prospective trial.Resuscitation 2010; 81: 1527-33. PMID: 20801576
- Nina Sviridova, Kenshi Sakai, Human photoplethysmogram: new insight into chaotic characteristics,Chaos, Solitons & Fractals, Volume 77, 2015, Pages 53-63,
ISSN 0960-0779, https://doi.org/10.1016/j.chaos.2015.05.005 (http://www.sciencedirect.com/science/article/pii/S0960077915001344) - Section 3: Cardiovascular physiology Chapter 33 Arterial pressure waveforms
![]()





































Epinephrine in cardiac arrest: the past, the present and the (im)possible future. Reflections after PARAMEDIC 2 trial.
23 JulThe past (a brief history of epinephrine use in cardiac arrest)
In 1901 Jokichi Takamine (1854-1922) isolated the pure form of adrenaline, also known as epinephrine.
Routine use of adrenaline for cardiac arrest was first proposed in the 1960’s. Its inclusion within cardiac arrest management was based upon an understanding of the physiological role of adrenaline, and experimental data from animal research which showed that ROSC was more likely when the drug was used.
Epinephrine was not included in cardiac arrest protocols on the basis of evidence of benefit in humans.
Epinephrine remained, since today, a significant component of advanced life support despite minimal human data indicating beneficial effect .
The rationale for use of epinephrine in cardiac arrest was that, in animal studies, increases aortic blood pressure and thus coronary perfusion pressure during chest compressions.
IMPORTANT, brief reminder on epinephrine effect and Coronary Perfusion Pressure.
Many and strong recent evidences demonstrates that “Among patients with OHCA, use of prehospital epinephrine was significantly associated with increased chance of return of spontaneous circulation before hospital arrival but decreased chance of survival and good functional outcomes
The Present: PARAMEDIC 2 trial.
G.D. Perkins, C. Ji, C.D. Deakin, et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest.
What kind of study is this:
Randomized, double-blind, multicentric.
Population
8014 patients with out-of-hospital cardiac arrest in the United Kingdom
Adult (>16 years) patients, transported by five National Health Service ambulance services in the United Kingdom, who had sustained an out-of-hospital cardiac arrest for which advanced life support was provided by trial-trained paramedics.
Apparent pregnancy, age of less than 16 years, cardiac arrest from anaphylaxis or asthma, administration of epinephrine before the arrival of the trial-trained paramedic.
Intervention
Paramedics administered either IV epinephrine 1mg every 3 – 5min + standard care or IV 0.9% normal saline bolus + standard care.
Comparison
Outcome
Results
Image attribution: REBEL Cast Ep56 – PARAMEDIC-2: Time to Abandon Epinephrine in OHCA?
Conclusions
In adults with out-of-hospital cardiac arrest, the use of epinephrine resulted in a significantly higher rate of 30-day survival than the use of placebo, but there was no significant between-group difference in the rate of a favorable neurologic outcome because more survivors had severe neurologic impairment in the epinephrine group.
Strengths
Limitations
What we know till today
Epinephrine in cardiac arrest improve ROSC and patients alive.
The improved survival is mostly due to patients with bad (<3 MRS) neurological outcome.
What that means
Administering the current recommended dose of Epinephrine we have to choose between numbers and quality of life.
Patients clearly said quality of life is more important
Epinephrine is anyway important because having bigger numbers of ROSC give the chance to improve neurological outcomes.
Future challenges
Understanding why epinephrine doesn’t work and can be detrimental on long term neurological outcome.
Obtaining more ROSC and better neurological outcomes in Cardiac Arrest
The (im)possible future
I think there are two key factors, in the actual way to use Epinephrine, that determine its failure:
The wrong administration route
When epinephrine is administered intravenously in a low flow state patient (as is a patient during cardiac arrest, even if proper chest compressions are performed), the amount of drug that arrives to perform the “local” alpha effect on arteries is just a minimal quantity of the (high!!!) dose. The major part rely in the venous circulation and is mobilized in great quantity only when ROSC happens determining a widespread vasoconstriction and a consequent “overdose” effect (think just at the “stunned” myocardium that has to overwhelm such ha great post-load work).
The wrong dose to the wrong patient
From the coronary perfusion pressure (CPP) point of view, every cardiac arrest patient is different: some patients have a (relative) good aortic pressure and a (relative) good coronary perfusione comparing to others.
When we administer the same amount of epinephrine to each of them this takes to an underdose in some patients (with low flow state) and an overdose in others (with good or high flow state).
So now what?
The right administration route
Probably the best route to administer epinephrine is not the vein but the artery.
It allows, even in a low flow state patient, a better chance to reach the vasoconstrictor effect maintaining a good aortic diastolic pressure and a consequent good coronary flow.
The right dose to the right patient
Giving epinephrine (standard dose) to a patient who has a low flow state (patients who need it more) make epinephrine usefulness (underdose) because just a little part of it circulate.
Giving epinephrine to patients in a good or high flow state (patients that need it less or don’t need epi at all) is detrimental and can cause overdose effect.
We need to know wich is the circulatory state of the patients to administer the right dose avoiding the “overdose” effect.
The only way to do this is monitoring aortic diastolic pressure through an arterial catheter. We can target Epinephrine dosage to reach a good aortic pressure maintaining a good CPP (achieving ROSC) and avoiding overdose.
Take home messages for future improvements in cardiac arrest management
Obtain an arterial line
Give Adrenaline intrarterially
Check blood pressure via arterial line
Target Adrenaline (doses and times) to maintain at least 40 mmHg of diastolic arterial pressure
References
Adrenaline and cardiac arrest. Ambulancetoday
G.D. Perkins, C. Ji, C.D. Deakin, et al.A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest
Rethinking Adrenaline in Cardiac Arrest- Jim Manning on Vimeo from SMACC Dub
Share this: